Femoral Acetabular Impingement
Summary
In femoral acetabular Impingement, either the femur or the acetabulum of the hip joint is not shaped quite right and therefore the hip does not move as smoothly as it should. This can cause damage to various hip structures including the tissue around the edge of the hip socket (labrum) and/or the smooth articular cartilage of the hip joint. This mechanical impingement can result in pain and decreased hip range of motion.
Treatment depends on severity of the disease, and non-operative treatment is usually recommended before pursuing surgery. Non-operative treatment includes physical therapy, pain medications, and activity modification to avoid activities that cause pain. If non-operative treatment is not sufficient, arthroscopic hip surgery to shave off the extra bone and smooth the articulating surfaces is recommended.
Clinical Presentation
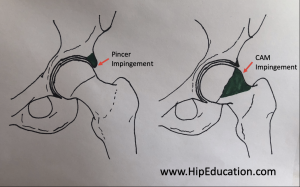
Femoral acetabular impingement results from excess bone formation on the surface of the femur and/or acetabulum, preventing smooth hip movement. There are two main types of femoral acetabular impingement, Cam and Pincer impingement. These are differentiated by which bone of the hip joint is causing the impingement. In the Cam type, the femoral head is not round enough, usually due to extra bone formation resulting in an uneven surface. The Pincer type occurs when the acetabulum has extra bone hanging over its edges, causing impingement with certain movements of the hip joint (figure 1). A combination of Cam and Pincer impingement can also occur.
Figure 1
The Cam type of impingement is more common in young males and the Pincer type is more common in middle-aged females. Although femoral acetabular impingement is equally likely in athletes and those who lead a more sedentary lifestyle, it may become symptomatic earlier in life in active individuals because of increased use of the hip joint.
The pain associated with femoral acetabular impingement is usually located in the groin area and is typically made worse by exercise, getting in and out of a car, leaning forward, and prolonged sitting. Pain is commonly described as a dull ache but can feel sharp or stabbing when performing complex movements such as twisting or squatting. Symptoms can also be referred to the side of the hip, the buttocks region or even the knee. In addition, individuals may complain of a stiff hip with limited range of motion, with or without pain. Another symptom includes a limp while walking, favoring the unaffected side.
Physical Exam
A common physical exam finding in femoral acetabular impingement is known as the C-sign. This is when the individual is asked to show where the pain is coming from and proceeds to form a “C” with their hand in order to cup it around the front of the affected hip. Another common finding, and the most sensitive physical exam maneuver for this condition, is a positive FADIR or anterior impingement test. A positive test means that pain is experienced when performing this test. FADIR is an acronym for flexion, adduction and internal rotation. As such, the doctor will bring the knee up toward the chest and rotate the hip inwards so the knee is pointing toward the opposite shoulder. In addition to pain, there will be limited range of motion seen while performing the FADIR test.
Imaging
X-rays are the initial imaging ordered when a diagnosis of femoral acetabular impingement is suspected. X-rays will reveal areas of excess bone, allowing for the identification of Cam and Pincer deformities. They may also show consequences of the disease such as osteoarthritis. An MRI can be obtained to better visualize damage that may have occurred to soft tissue structures of the hip such as the articular cartilage and labrum. A special dye needs to be injected directly into the hip joint for the MRI. A freezing medication may also be injected into the joint at the same time. If the medication relieves the pain, this will confirm that the hip pain is a result of femoral acetabular impingement.
Non-operative Treatment
Femoral acetabular impingement does not resolve on its own and in time, further damage to the hip joint structures will occur without treatment. In general, various non-operative treatments are recommended before surgical intervention is considered. One common non-operative treatment is activity modification. This involves limiting, changing or avoiding activities that worsen pain. On occasion, it is challenging to effectively modify activities for various reasons. This is a major factor in deciding whether to pursue surgery or not. Pain medications such as ibuprofen and other NSAIDs can also help to control the pain. Additionally, physical therapy and a home exercise program may be recommended to strengthen the muscles around the hip joint and improve range of motion. This can lead to reduced pain and increased function in the affected hip.
Operative Treatment
Surgery for femoral acetabular impingement is typically performed if there is damage to the joint structures, such as a tear of the labrum, or evidence of osteoarthritis. Surgery is also performed if non-operative management is not successful. There are two main surgical treatments that can be performed depending on the extent of the disease. These are arthroscopic hip surgery and surgical hip dislocation.
Hip Arthroscopy
Arthroscopic hip surgery has become the surgery of choice to treat femoral acetabular impingement in many hospitals because it is less invasive compared to open surgery. It involves the use of a small camera and other instruments inserted into the hip joint through incisions in the skin. The surgeon can repair or remove damaged articular cartilage and labrum as well as trim the excess bone off the femoral head or acetabulum.
Surgical Hip Dislocation
This technique involves performing the same procedures of trimming bone and repairing or removing damaged tissue as seen in hip arthroscopy. However, it differs in that it is performed by exposing both the head of the femur and surface of the acetabulum by temporarily dislocating the hip. Surgical hip dislocation may be favored over arthroscopy in cases where the impingement is complex and involves harder to access areas of the hip. In patients over 60 years of age who have femoral acetabular impingement in addition to osteoarthritis, a total hip replacement may be a better surgical option.