Femoral Neck Fracture
Summary
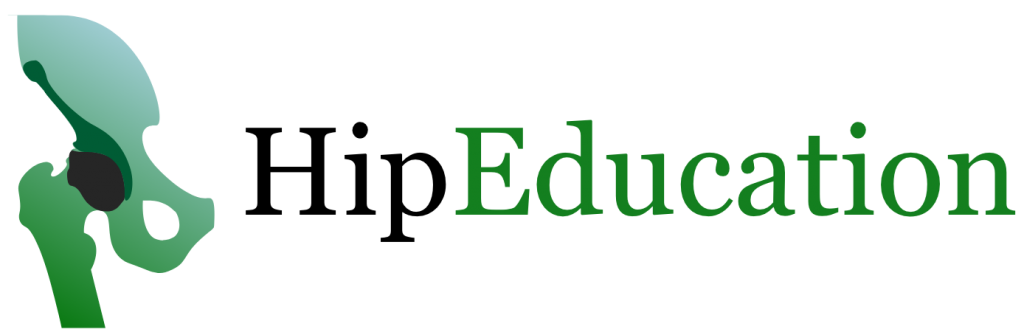
A femoral neck fracture is a fracture of the femur in the area just below the “ball” of the hip joint, or head of the femur (Figure 1). This area is called the femoral neck and connects the shaft of the femur to its head. These fractures usually occur in older patients as a result of a fall onto the hip. In addition to pain and an inability to stand or walk, a potentially serious long-term consequence is bone death (avascular necrosis) of the femoral head. This results in hip arthritis due to a disruption in the hip’s blood supply, which runs along the femoral neck.
Treatment of a femoral neck fracture is largely surgical with the overarching goals of minimizing pain, restoring function, and preventing avascular necrosis. Surgery requires either stabilizing the femoral neck fracture using screws (hip pinning) or removing the hip joint completely and replacing it with an artificial hip -either a partial hip replacement or a total hip replacement. The choice of surgery depends on the state of the local blood supply, age of the patient, and nature of the fracture.
Figure 1
Clinical Presentation
A femoral neck fracture most often results from a recent fall on the affected hip. It commonly occurs in older patients with weaker bone (Osteoporosis), although it can occur in younger patients who suffer higher impact injuries. Patients will have pain in the hip and will typically find it difficult or impossible to put weight on the injured leg. If they can weight-bear, they will have a limp that favors the unaffected hip. In addition, there is usually bruising of the skin and swelling in the area around the fracture. The affected leg will appear shorter if the two ends of the fracture are not aligned, and will also be externally rotated.
Women above the age of 65 are most susceptible to femoral neck fractures. This is because older women are most affected by osteoporosis, which results in weakening of the bones over time. When a young person presents with a femoral neck fracture, it is usually due to a “high energy injury” such as a car accident or fall from a high place that placed significant force on the femur. In contrast, elderly individuals often sustain femoral neck fractures by falling from ground level because aged bones break under far less force.
An additional risk factor includes the use of medications that decrease the strength of the bone, or bone mineral density. These include heparin, anticonvulsants, methotrexate, and glucocorticoids.
Physical Exam
On physical exam, a femoral neck fracture will cause pain when the doctor moves the hip in various directions. There will also be pain when pressing on (palpating) the area around the hip joint. In rare instances, nearby nerves may be injured. The doctor may observe weakness of the thigh or other lower leg muscles and numbness, tingling, or complete loss of sensation over different areas of the leg depending on which nerves are impacted.
Imaging
The first line of imaging for a suspected femoral neck fracture is an x-ray. Considering bone is well-visualized on x-ray, a displaced fracture or one with a clear fracture line will be easily seen. The x-ray will reveal if the fracture is well-aligned (non-displaced) or if the two ends of the fracture are not matched up (displaced). The doctor will also be able to determine if the fracture is in many pieces (comminuted), or if there is a clean break resulting in a single fracture line (non-comminuted). Sometimes, a fracture will not show up on x-ray because it is a stress fracture, or only a small crack in the bone has occurred. In this situation an MRI or CT can be useful tools.
Non-operative Treatment
In most cases, a femoral neck fracture is best treated with surgery. However, there may be rare instances where an incomplete stress fracture or a stable non-displaced fracture is treated non-surgically. In addition, elderly patients may have medical issues that prevent safe surgery. However, foregoing surgical treatment of a femoral neck fracture can lead to failure of the fractured ends of the bone to heal (nonunion) and may increase the chance of developing bone death. Femoral neck fractures often lead to a period of minimal or no walking and the associated muscle atrophy that this type of prolonged immobilization brings can be its own issue.
In all other patients, surgery is indicated. For these patients treatment before surgery includes not placing weight on or unnecessarily moving the affected hip to prevent further damage to the bone. Pain medications can also be given prior to surgery to help alleviate symptoms, such as NSAIDs. In some cases, a local pain medication is injected into the area of the fracture for temporary pain management, called a localized nerve block.
Operative Treatment
Surgery is the most effective and successful intervention for treatment of a femoral neck fracture. There are two different types of surgeries that are commonly used in the treatment of femoral neck fractures: hip pinning and hip replacement. The type of surgery performed depends on the characteristics of the fracture and the age and activity level of the patient.
Hip Pinning
Typically, if the fracture is well-aligned (non-displaced) and/or occurs in a younger person, it can be treated with hip pinning (figure 2). Hip pinning to stabilize a fractured femoral neck involves the placement of three screws perpendicular to the fracture line to join the head of the femur to the neck.
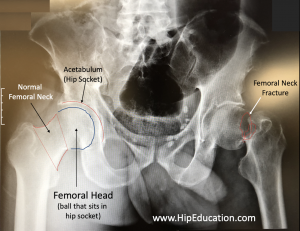
Figure 2: Hip Pinning

Hip Replacement (Partial Hip Replacement or Total Hip Replacement)
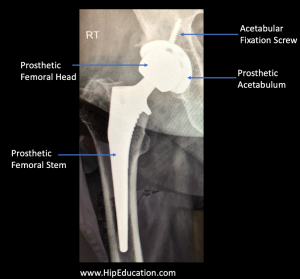
If the femoral neck fracture is displaced and occurs in an older person, a partial or total hip replacement is usually a better option than hip pinning. Traditionally, a partial hip replacement has been performed to treat displaced femoral neck fractures in older individuals. This procedure involves cutting through the femoral neck below the fracture site, removing the femoral head and inserting a prosthesis into the thigh bone (figure 3). In persons with pre-existing hip arthritis or a higher activity level it may be preferable to treat a displaced femoral neck fracture with a total hip replacement -which includes inserting a femoral prosthesis to replace the ball-part of the joint AND replacing the matching acetabulum (figure 4). Both partial and total hip replacements usually allow patients to begin weight-bearing immediately after surgery.
Figure 3: Partial hip replacement (hemiarthroplasty)
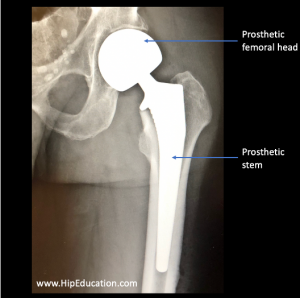
Figure 4: Total hip replacement (arthroplasty)
Patient Reference Websites