Slipped Capital Femoral Epiphysis
Summary
Slipped capital femoral epiphysis (SCFE) is a disease of the hip that occurs shortly after the onset of puberty. The growth plate (physis) located between the femoral head (epiphysis) and femoral neck is made of cartilage that expands and hardens to form new bone as the child grows. This site is not as strong as bone, making it a weak point where the two pieces of bone on either side can become misaligned.
It is not clear what exactly causes this condition to develop, though childhood obesity is a major risk factor and males are more often affected than females. Slippage of the epiphysis off of the femoral neck can cause pain and limited range of motion in the affected hip. If left untreated, this can progress to abnormal bone growth and a difference in leg-lengths between the affected and unaffected sides among other long-term consequences. X-rays are the imaging that is most often used to determine the presence of slipped femoral capital epiphysis, though an MRI may be useful in certain cases.
Once diagnosed, the goal of treatment is to stabilize the hip and decrease the risk of further slippage in order to prevent future complications as the child grows. The treatment of choice is surgical insertion of a single highly specialized screw that travels through the growth plate to connect the head and neck of the femur, holding them in alignment while the child continues to grow.
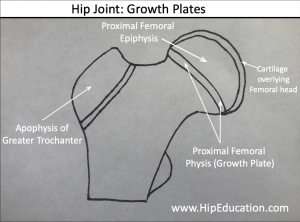
Figure 1: Drawing of the femoral head showing the location of the growth plate
Clinical Presentation
In a growing child, there are growth plates (physis) located at each end of the femur. The growth plate at the hip joint end of the femur is located between the femoral head (epiphysis) and femoral neck (figure 1). Growth plates are composed of specialized cartilage that expands length-wise and eventually turns into new bone, allowing the bone to grow longer as the child gets older.
In slipped femoral capital epiphysis, the head of the femur on one side of the growth plate slides or “slips” off the femoral neck on the other side of the growth plate, typically in a backwards direction. This slippage occurs through the growth plate, which is weaker than bone. The exact cause of this slippage is unknown.
Slipped Capital Femoral Epiphysis occurs in young adolescents, usually shortly after the onset of puberty. Puberty occurs at different ages for males and females. The most common age of pubertal onset for males is between 13-15 years and for females is between 11-13 years. Males are 2.5 times more likely to be affected by slipped capital femoral epiphysis than females. Additionally, the single greatest risk factor for developing the disease is obesity. In around 50% of adolescents, the disease occurs in both hips.
The most common symptom is pain, occurring most often in the groin or the front of the thigh. The pain can be referred to areas further down the thigh or even to the knee. Initial symptoms can sometimes develop after a fall or other traumatic event. The adolescent’s parents may also notice a limp that is made worse by activity and external rotation of the affected leg compared to the normal leg.
Physical Examination
In slipped capital femoral epiphysis, it is not unusual for adolescents to be overweight. The affected leg or legs can be turned outward (externally rotated) and an abnormality is often noticeable in the way the child walks. There may also be limitations in range-of-motion of the hip with testing, which is particularly pronounced with internal rotation.
The affected hip is usually quite painful, especially at the limits of range of motion and the patient may involuntarily flex their muscles to prevent movement (guarding). Another finding on physical examination is shortening of the affected leg as a result of the slippage. This shortening can be up to 1-3 cm compared to the unaffected leg. All these changes in the position of the hip due to the slippage can result in a limp. If the condition is severe enough, the patient will be unable to put weight through the hip.
Imaging
X-rays are the main imaging used in the diagnosis of slipped capital femoral epiphysis. They can be used to determine the presence and extent of the slip between the femoral head and neck. On rare occasions, the degree of slippage will be minor enough that it is not perceived on x-ray. An MRI, which provides a more detailed image of the soft tissue such as muscles and ligaments, may be used to help confirm the diagnosis in these cases.
Non-operative Treatment
The main intervention for the treatment of slipped capital femoral epiphysis is surgical. Once the diagnosis is made however, it is important to avoid weight bearing on the affected hip until the surgery is performed. Temporary treatment of pain that may be present as a result of the condition includes NSAIDs and other pain medications.
Operative Treatment
The goal of treatment is to stabilize the hip using hardware to maintain correct positioning of the femoral head and neck with respect to each other. Stabilization prevents any further slippage and may minimize the potential complications that can accompany a slipped capital femoral epiphysis. Complications that can occur from a SCFE include osteonecrosis, chrondrolysis, permanent changes in bone structure resulting in abnormalities with walking, leg length discrepancy, early osteoarthritis, labrum tears, and/or damage to other joint structures.
Surgical stabilization of the femoral head on the femoral neck involves the placement of a single specialized screw into the femur, connecting the neck and head through the growth plate. Following the surgery, there will be some restrictions placed on activity until the growth plate closes, typically lasting 6-9 months. Occasionally, individuals with very severe disease may require more specialized surgeries such as a femoral osteotomy. An osteotomy involves removal of part of the bone, in this case part of the femur, to better align the hip joint and ensure proper healing.
Research is ongoing to determine the appropriateness of preventative screw insertion in the unaffected hip in those suffering from slipped capital femoral epiphysis of 1 hip. This is because up to 50% of individuals who are diagnosed with slipped capital femoral epiphysis in one hip will develop it in the opposite hip.